
The loss of a pregnancy can be a very traumatic experience for couples. Studies indicate that over one-fifth of women who experience a pregnancy loss show symptoms of anxiety and depression. When a single pregnancy loss can have such traumatizing effects, recurrent pregnancy loss (RPL) can have devastating psychological effects.
Recurrent miscarriage, also known as recurrent pregnancy loss, is generally defined as the occurrence of two or more consecutive pregnancy losses before 20 weeks of gestation. This phenomenon impacts about 1-2% of reproductive-age women and carries significant physical and emotional consequences (Practice Committee of the American Society for Reproductive Medicine, 2012). Unlike isolated miscarriages, which are often attributed to random chromosomal abnormalities, recurrent miscarriages are more likely due to underlying pathologies. One of the first things that needs to be addressed is when the patient is experiencing her miscarriages. Miscarriages experienced at different gestation periods may indicate different factors. Understanding these causes helps guide effective management and support for affected couples.
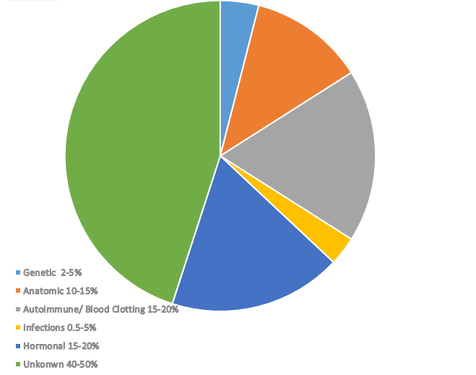
While there are a number of established factors that can be linked to repeated pregnancy losses, causes of almost half of recurrent pregnancies still remain a mystery. Together, autoimmune factors, hormonal problems and problems with blood clotting make up for almost 70% of all known causes. Therefore, when a woman goes through a number of miscarriages, the starting point for testing would usually involve one of these three domains.
Reasons Behind Consecutive Miscarriages
The following causes (in no specific order) are known to be involved with repeated pregnancy losses:
1. Genetic Factor
Genetic causes make up of 2-5 percent of all miscarriages. Among genetic causes, chromosomal abnormalities are the leading genetic cause of miscarriage, accounting for approximately 50-60% of early pregnancy losses that occur for genetic reasons. These abnormalities include both numerical and structural chromosomal defects.
A. Aneuploidy
Aneuploidy, an abnormal number of chromosomes, is one of the most common causes of miscarriage. Trisomy (the presence of an extra chromosome) is the most frequent aneuploidy observed, particularly trisomies of chromosomes 16, 21, and 22. Monosomy X (Turner syndrome) is also prevalent among miscarriages but is rarely viable beyond the first trimester (Hassold & Hunt, 2001). Aneuploidies often occur due to meiotic nondisjunction, a process in which chromosomes fail to separate correctly during cell division in gametes, leading to embryos with abnormal chromosomal content (Nagaoka et al., 2012).
B. Structural Chromosomal Abnormalities
Structural chromosomal abnormalities, including translocations, inversions, and deletions, also contribute to recurrent miscarriage. Translocations occur when chromosome segments are rearranged between non-homologous chromosomes. Balanced translocations, which do not result in a net gain or loss of genetic material, may not affect the individual but can lead to miscarriages if the rearranged chromosomes disrupt embryo development (Stephenson et al., 2002). Parental karyotype analysis can often reveal structural abnormalities in couples with recurrent pregnancy loss.
C. Genetic Syndromes and Single-Gene Mutations
While chromosomal abnormalities are significant, single-gene mutations or genetic syndromes can also increase miscarriage risk.
C1. Inherited Genetic Syndromes
Inherited genetic conditions, including autosomal recessive or autosomal dominant syndromes, can contribute to pregnancy loss. For example, mutations in the FOXL2 gene, associated with Blepharophimosis-Ptosis-Epicanthus Inversus syndrome, can lead to ovarian dysfunction, increasing miscarriage risk (Crisponi et al., 2001).
C2. Thrombophilia-Associated Gene Mutations
Specific gene mutations that cause thrombophilia, or increased blood clotting, have been linked to miscarriages. Mutations in genes such as F5 (Factor V Leiden) and F2 (prothrombin) can lead to abnormal blood clotting in the placenta, impairing blood flow and ultimately causing miscarriage (Rey et al., 2003). Although thrombophilia is a multifactorial condition, genetic predisposition is a contributing factor in some recurrent pregnancy losses.
D. Epigenetic Factors and Parental Age
Epigenetic changes, heritable modifications in gene expression that do not involve changes in the DNA sequence, also contribute to miscarriage risk. DNA methylation errors, for instance, can disrupt gene expression in the embryo, leading to developmental arrest and miscarriage.
D1. Parental Age
Advanced maternal and paternal ages are associated with increased risks of genetic abnormalities, primarily due to an accumulation of mutations in germ cells over time. Women over 35 are at a higher risk of producing oocytes with chromosomal errors, leading to miscarriages (Hassold & Chiu, 1985). Similarly, advanced paternal age has been linked to DNA fragmentation in sperm, which can increase miscarriage risk due to abnormal embryo development (Kumar et al., 2012).
D2. Imprinting Disorders
Imprinting disorders, where certain genes are expressed in a parent-of-origin-specific manner, are linked to miscarriage risk. Errors in imprinting can lead to disorders such as Prader-Willi syndrome or Angelman syndrome, which can result in miscarriages or adverse pregnancy outcomes (Chong & Hutchinson, 2000).
Advances in genomic technologies have greatly enhanced the understanding of genetic causes of miscarriage. High-throughput sequencing, chromosomal microarray analysis (CMA), and preimplantation genetic testing (PGT) allow for detailed chromosomal and genetic analysis of embryos and parents.
1. Chromosomal Microarray Analysis (CMA)
CMA has replaced karyotyping in many clinics as the primary test for identifying chromosomal abnormalities in miscarriage tissue. This technology detects submicroscopic chromosomal imbalances that traditional karyotyping may miss, providing insight into the causes of unexplained miscarriages (Reddy et al., 2012).
2. Next-Generation Sequencing (NGS)
NGS has facilitated the identification of single-gene mutations and small-scale genetic abnormalities that contribute to miscarriage. It has also helped in discovering novel genes associated with early pregnancy loss, providing further insights into genetic causes (Xu et al., 2020). When patients experience multiple pregnancy losses, an IVF cycle involving NGS testing becomes a very effective tool. This is not only done for recurrent miscarriages, but it also is an effective tool for repeated IVF failures.
2. Anatomical Abnormalities
Structural anomalies within the reproductive tract can impair implantation, disrupt normal fetal development, or lead to placental insufficiency, all of which can contribute to an undesired event of miscarriage. It has been estimated that anatomical abnormalities contribute up to 15% of all miscarriages.
• Congenital Uterine Anomalies: Uterine malformations, such as septate, bicornuate, or unicornuate uterus, can increase the risk of miscarriage. A septate uterus, where a fibrous septum divides the uterine cavity, is particularly associated with high miscarriage rates. The septum may not support adequate blood flow to the implanted embryo, leading to placental insufficiency and pregnancy loss (Grimbizis et al., 2001). Surgical correction of the septum has been shown to improve pregnancy outcomes.
• Acquired Uterine Abnormalities: Conditions such as fibroids (particularly submucosal fibroids that distort the uterine cavity) and intrauterine adhesions (scarring within the uterus, often a result of prior surgeries or infections) can interfere with implantation or fetal development. These structures can distort the shape of the uterine cavity, reduce space, and limit blood flow to the developing embryo, thereby increasing the risk of miscarriage (Saravelos et al., 2008).
3. Endocrine Disorders (Hormonal Problems)
Endocrine abnormalities are well-documented contributors to recurrent pregnancy loss, primarily due to their impact on hormonal balance and uterine receptivity. Hormonal issues are known to play a role in 15-20% of recurrent miscarriages.
• Polycystic Ovary Syndrome (PCOS): PCOS is a common endocrine disorder characterized by irregular ovulation, hyperandrogenism, and insulin resistance. Elevated insulin levels in women with PCOS can lead to poor endometrial development and may contribute to early pregnancy loss (Boomsma et al., 2006). Furthermore, the hormonal imbalance associated with PCOS can disrupt the luteal phase (the period after ovulation when the endometrium prepares for embryo implantation), potentially leading to an inadequate uterine environment for implantation.
• Luteal Phase Defect: The luteal phase, regulated by progesterone produced by the corpus luteum after ovulation, is critical for maintaining an optimal endometrial environment for implantation and early embryo support. A deficiency in progesterone production, known as luteal phase defect, can lead to insufficient endometrial preparation, impairing implantation and increasing the risk of miscarriage.
• Thyroid Disorders: Thyroid function plays a significant role in pregnancy maintenance. Hypothyroidism (underactive thyroid) can lead to insufficient production of thyroid hormones, which are essential for fetal development, especially in the first trimester when the fetus relies on maternal thyroid hormones. Even in euthyroid women (normal thyroid function), the presence of thyroid autoantibodies, particularly thyroid peroxidase (TPO) antibodies, is associated with a 2-3-fold increased risk of miscarriage (Thangaratinam et al., 2011). These antibodies may affect the maternal immune system, impairing the uterine environment.
4. Immunological Factors
The immune system must adapt to support pregnancy, as the fetus is genetically distinct from the mother. Disruptions in this adaptation can lead to miscarriage.
• Antiphospholipid Syndrome (APS): APS is an autoimmune condition characterized by the presence of antiphospholipid antibodies, such as lupus anticoagulant and anticardiolipin antibodies. These antibodies increase the risk of clot formation within blood vessels, including those in the placenta. Placental clots reduce oxygen and nutrient delivery to the fetus, leading to miscarriage. APS is a well-documented cause of recurrent pregnancy loss, and its management typically involves anticoagulation therapy (Rai et al., 2005).
• Natural Killer (NK) Cell Abnormalities: NK cells play a role in early pregnancy, assisting in placental development. Elevated levels of NK cells or abnormal NK cell function are hypothesized to contribute to recurrent miscarriage, as overactive NK cells may attack placental cells. However, the exact role of NK cells in miscarriage is still debated, with conflicting evidence on whether NK cell modulation improves pregnancy outcomes (Quenby et al., 2009).
5. Thrombophilic Disorders
Inherited thrombophilias are genetic conditions that predispose individuals to abnormal blood clotting, which can have adverse effects during pregnancy.
• Factor V Leiden Mutation: This mutation leads to resistance to activated protein C, a crucial anticoagulant, resulting in a hypercoagulable state. During pregnancy, this mutation can lead to placental thrombosis (clot formation in the placenta), impairing fetal oxygen and nutrient supply, which may cause miscarriage, particularly in the second trimester (Preston et al., 2002).
• Prothrombin Gene Mutation: This mutation also promotes a hypercoagulable state, increasing the risk of placental blood clots. Women with this mutation have a higher risk of miscarriage, especially late in pregnancy.
• Protein C and S Deficiencies: Protein C and S are natural anticoagulants. Deficiencies in these proteins lead to increased clot formation, which can compromise placental function. However, the link between thrombophilias and early miscarriages remains controversial, with some studies suggesting they are more relevant to late pregnancy complications (Lockwood, 2002).
6. Lifestyle and Environmental Factors
Several modifiable lifestyle factors can impact pregnancy outcomes.
• Smoking: Nicotine and other toxins in cigarette smoke impair uterine blood flow, creating a hypoxic (low oxygen) environment that can disrupt embryo development and increase miscarriage risk. Smoking is associated with a higher risk of chromosomal abnormalities in the embryo, possibly due to oxidative stress from tobacco (Green et al., 2007).
• Alcohol and Caffeine Intake: Excessive alcohol consumption is associated with fetal toxicity, which can contribute to miscarriage. High caffeine intake (typically above 200-300 mg per day) has been linked to increased miscarriage risk, potentially due to its effects on the cardiovascular and hormonal systems that support pregnancy (Ford & Schust, 2009).
• Obesity: Obesity is associated with a higher risk of miscarriage due to hormonal imbalances, increased insulin resistance, and chronic low-grade inflammation. Obesity can also impair endometrial receptivity, which is crucial for successful implantation and pregnancy maintenance (Metwally et al., 2008).
7. Infections
Certain infections can increase the risk of miscarriage by causing inflammatory responses that damage fetal tissues or disrupt the maternal-fetal interface. While infective causes are often likely to induce a pregnancy loss during the active phase, some infections can cause chronic issues that can be a factor for recurrent miscarriages:
• Chlamydia trachomatis and Ureaplasma urealyticum: These bacteria can cause chronic endometritis, an inflammation of the uterine lining, which may impair implantation or disrupt placental function, leading to miscarriage. Chronic infection with these bacteria has been associated with adverse pregnancy outcomes, though evidence linking them specifically to recurrent miscarriage is mixed (Baud et al., 2008).
• Cytomegalovirus (CMV): CMV is a herpesvirus that can be transmitted to the fetus if the mother is infected during pregnancy. Fetal CMV infection can lead to developmental abnormalities and increase the risk of miscarriage, particularly when infection occurs early in pregnancy. This is likely to be an issue in the active phase of the infection.
8. Unexplained Causes
Approximately half of all recurrent miscarriages remain unexplained despite thorough evaluation. Unexplained recurrent miscarriages may involve subtle abnormalities in immune, genetic, or hormonal function that current diagnostic tests cannot detect. Additionally, multifactorial causes are likely in many cases, where minor abnormalities in multiple systems collectively contribute to pregnancy loss (Coomarasamy et al., 2014). In some cases, even though there is no known cause, certain prophylactic measures can be taken, and we observe positive results with these measures, which shows that even though certain problems may not show up on labs, they may still respond to anticoagulation, corticosteroids, antibiotics and other prophylactic measures.
References
• Baud, D., Regan, L., & Greub, G. (2008). Emerging role of Chlamydia and Chlamydia-like organisms in adverse pregnancy outcomes. Current Opinion in Infectious Diseases, 21(1), 70-76.
• Boomsma, C. M., Fauser, B. C., & Macklon, N. S. (2006). Pregnancy complications in women with polycystic ovary syndrome. Seminars in Reproductive Medicine, 24(1), 35-43.
• Chong, S., & Hutchinson, W. (2000). The role of genomic imprinting in development and disease. The Lancet, 355(9197), 2117–2122.
• Coomarasamy, A., et al. (2014). PROMISE trial: effects of progesterone in recurrent miscarriages. Health Technology Assessment, 18(40), 1-70.
• Crisponi, L., Deiana, M., Loi, A., et al. (2001). The putative forkhead transcription factor FOXL2 is mutated in blepharophimosis/ptosis/epicanthus inversus syndrome. Nature Genetics, 27(2), 159–166.
• Ford, H. B., & Schust, D. J. (2009). Recurrent pregnancy loss: etiology, diagnosis, and therapy. Reviews in Obstetrics and Gynecology, 2(2), 76-83.
• Grimbizis, G. F., et al. (2001). Uterine malformations and hysteroscopic treatment outcomes. Human Reproduction Update, 7(2), 161-174.
• Green, K. A., et al. (2007). Smoking and miscarriage: a systematic review. Tobacco Control, 16(2), 120-124.
• Hassold, T., et al. (2007). The origin of human aneuploidy. Human Molecular Genetics, 16(R2), R203-R208.
• Kumar, N., Singh, A. K., & Yadav, P. (2012). Male infertility: An overview of genetic aspects. Journal of Postgraduate Medicine, 58(3), 243–249.
• Lockwood, C. J. (2002). Mechanisms of endometrial bleeding. Menopause, 9(6), 411-417.
• Metwally, M., et al. (2008). Impact of obesity on female reproductive function. Obesity Reviews, 9(5), 456-468.
• Nagaoka, S. I., Hassold, T. J., & Hunt, P. A. (2012). Human aneuploidy: Mechanisms and new insights into an age-old problem. Nature Reviews Genetics, 13(7), 493–504.
• Practice Committee of the American Society for Reproductive Medicine. (2012). Definitions of infertility and recurrent pregnancy loss. Fertility and Sterility, 98(3), 1-2.
• Preston, F. E., et al. (2002). Increased fetal loss in women with thrombophilia. The Lancet, 356(9225), 270-273.
• Quenby, S., et al. (2009). Pre-implantation endometrial leukocytes in women with recurrent miscarriage. Human Reproduction, 14(8), 2386-2391.
• Rai, R., et al. (2005). Antiphospholipid antibodies in recurrent miscarriage. Human Reproduction, 10(7), 1818-1823.
• Reddy, U. M., Page, G. P., & Saade, G. R. (2012). The role of DNA microarrays in the evaluation of fetal death. American Journal of Obstetrics and Gynecology, 207(4), 279–288.
• Rey, E., Kahn, S. R., David, M., & Shrier, I. (2003). Thrombophilic disorders and fetal loss: A meta-analysis. Lancet, 361(9361), 901–908.
• Saravelos, S. H., et al. (2008). Pattern of pregnancy loss in uterine anomalies. Reproductive BioMedicine Online, 17(1), 134-138.
• Stephenson, M. D., Awartani, K. A., & Robinson, W. P. (2002). Cytogenetic analysis of miscarriages from couples with recurrent miscarriage: A case-control study. Human Reproduction, 17(2), 446–451.
• Thangaratinam, S., et al. (2011). Thyroid autoantibodies and miscarriage risk. British Medical Journal, 342, d2616.
• Xu, Y., Li, L., Zhang, H., et al. (2020). Clinical application of whole-exome sequencing in recurrent pregnancy loss. Journal of Clinical Medicine, 9(4), 1156.