
Before proceeding with treatment, it is very important that the male patient has been evaluated by his urologist and the precise reason for azoospermia has been established, whether obstructive or non-obstructive. Similarly, a post-ejaculate urinalysis is an important test to administer azoospermic men so that retrograde ejaculation can be ruled out as a possible explanation for azoospermia. If you are diagnosed with retrograde ejaculation, very simple methods of sperm isolation from your urine can be applied and the isolated sperm cells can be used for IVF treatment. A physical examination will also be indicative of possible causes of azoospermia. For instance, men with normal testes volume with bilaterally indurated epididymis or absent vas deferens can be identified as being azoospermic of obstructive etiology. On the other hand, presence of low testes volume and a history of cryptorchidism will indicate a case of azoospermia with non-obstructive etiology.
With recent innovations in medical technologies, surgical sperm extraction methods have become available. With any sperm retrieval procedure, there are three main goals to prioritize:
-To obtain the best quality of sperm possible with the surgical procedure. Given that the sperm sample which will be obtained will not contain mature spermatozoa found in normal sperm ejaculate, the surgeon still needs to do his best to retrieve the sperm cells that may be as close to the mature spermatozoa as possible, if the patient has viable sperm cells.
-To obtain a sufficient amount of sperm for fresh use during the IVF cycle and possibly for cryopreservation for a future cycle. Even though this is a very minor procedure, it is still a surgical procedure, so if possible, the procedure should aim to retrieve enough sperm for a few IVF cycles.
-To make sure that there is minimal damage to the reproductive tract when obtaining the sperm sample surgically so that future attempts at surgical sperm retrevial/extraction are not jeopardized.
Surgical sperm collection methods include the following:
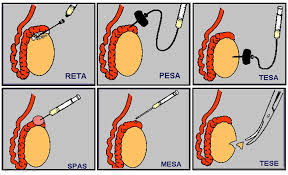
1- Percutaneous Epididymal Sperm Aspiration (PESA)
PESA is a simple method of sperm extraction used for men who have an obstruction of the vas deferens, either due to vasectomy or other obstruction. In order to minimize scarring, PESA is usually done on one side. Although the sperm obtained with this procedure will be immature and lower quality sperm, majority of the time, PESA will yield enough sperm cells for the ICSI procedure. You should also keep in mind that the longer the time period you have been exposed to the obstruction, the lower the quality and quantity of sperm that can be obtained with this method. Therefore, younger patients often respond better to this method compared to men in more advanced age brackets. Similarly, although PESA yields good results for patients with vasectomy, the duration after vasectomy can be decisive whether a good sample is likely to be obtained.
2- Micro Epididymal Sperm Aspiration (MESA)
MESA sperm retrieval technique involves aspiration of sperm from the epididymis with a fine needle, which is a more advanced version of the PESA procedure. It is a surgical procedure and is carried out under a general anesthetic. Sperm extracted using this technique are often of poor quality but are usually suitable for freezing. In some cases, enough sperm might be collected for a number of ICSI procedures, allowing the patients to use part of the sperm for the ongoing fresh cycle and preserve some of it for a future cycle.
3- Testicular Sperm Extraction (TESE)
This method of sperm extraction is often used for non-obstructive type of azoospermia where sperm cannot be obtained from the epididymis. TESE procedure requires taking a small piece of tissue from the testis and isolating the sperm from this tissue. Compared to MESA or PESA, a lower number of sperm cells are likely to be extracted, and in some cases, viable sperm may not be found in the biopsy tissue, which may require canceling the cycle or opting for sperm donation.
It should be known that sperm samples extracted/retrieved via surgical methods will not be as mature as spermatozoa found in the ejaculate, therefore, success rates with surgically obtained sperm samples are likely to be lower compared to standard sperm samples. Furthermore, while in some cases it may appear that freezing the surgically obtained sample may be an option, viability of this sample is likely to be further reduced with the freeze/thaw procedures. It is always a good idea to use surgically retrieved sperm cells when they are fresh.
The diagram below shows how each of the surgical sperm retrieval methods are administered:
You may also be interested in our “Stem Cell Therapeutical Study” for Non-Obstructive Azoospermia.